

Introduction
Acute coronary syndromes (ACS) are a group of conditions referring to cardiac ischaemia where part of the heart muscle is unable to function properly or infarcts. It includes:
- Unstable angina (angina at rest or minimal effort)
- Non- ST elevation myocardial infarction (NSTEMI), which has at least 2 of: symptoms at rest, raised troponin level, ECG changes
- ST elevation myocardial infarction (STEMI): NSTEMI features with ST elevation on ECG
Epidemiology
ACS is the commonest cause of death in the UK. 50% of deaths occur within 2 hours of onest.
Causes
Atherosclerosis accounts for most cases. Ischaemia is triggered by rupture or erosion of the fibrous cap of a coronary artery plaque.
Risk factors
Modifiable
- Smoking
- Hypertension
- Diabetes
- Hyperlipidaemia
- Obesity
- Sedentary lifestyle
Non-modifiable
- Age
- Male
- Family history
Pathophysiology
Ischaemia from atherosclerosis occurs due to either:
- Fibrous cap of atherosclerotic plaque gets a superficial injury and a thrombus forms on it
- Fibrous cap completely ruptures, so a thrombus forms within the cap and tis contents escape
Platelets aggregate and release serotonin and thromboxane A2, causing vasoconstriction and further reducing coronary perfusion.
Pathology by ACS type
- Unstable angina: Ischaemia but no injury. Angina may progress to infarction if occlusion persists.
- NSTEMI: Subendocardial infarction
- STEMI: Transmural infarction
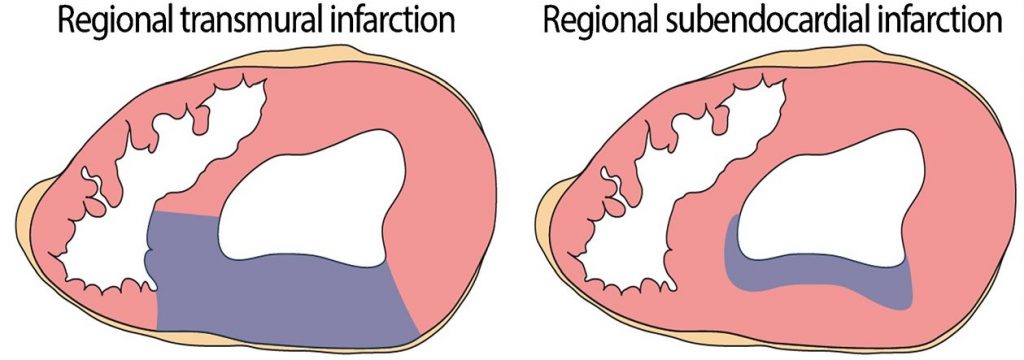
STEMIs lead to transmural infarcts. NSTEMIs lead to subendocardial infarcts
Clinical features
Symptoms
Chest pain is the most important symptom. The pain is similar to angina but lasts longer and is more severe.
Chest pain is typically central, crushing in character, lasts for over 20 minutes and may radiate to the jaw, neck, shoulders or arms (usually inner part of left arm).
Other symptoms include:
- Shortness of breath
- Sense of impending doom
- Nausea and vomiting
- Syncope
- Vomiting (especially in inferior MI)
Sudden death may occur due to asystole or ventricular fibrillation, especially within the first hour of symptom onset.
Silent myocardial infarction refers to MIs with no or atypical symptoms; these may present in elderly and/or diabetic patients. They can be incidentally diagnosed using ECG or lab tests.
Signs
Sympathetic activation leads to:
- Pallor
- Sweating
- Tachycardia
Impaired myocardial function produces:
- Shortness of breath
- Lung crackles
- Raised JVP
- S3 and S4 heart sounds
- Cold peripheries
- Peripheral oedema
- Cyanosis
- Hypotension
Vagal activation can occur in inferior infarcts, producing:
- Vomiting
- Bradycardia
Fever commonly occurs from the inflammatory response triggered by infarction. ACS can also present with complications of infarction e.g. pericarditis, mitral regurgitation.
Investigations and diagnosis
ACS type diagnosis
ACS diagnosis dictates management and is based on:
- Suggestive history
- ECG changes
- Blood markers of myocardial injury e.g. troponins
Unstable angina: symptoms/signs of MI ± ECG changes of ischaemia
NSTEMI: symptoms/signs of MI + Raised blood markers ± ECG changes of ischaemia
STEMI: symptoms/signs of MI + Raised blood markers + ST elevation on ECG
In reality, the above types of ACS form a continuum rather than being discrete entities.
First-line investigations
ECG (perform ASAP):
Ischaemia (in unstable angina and NSTEMI) may produce ST depression and T wave changes.
STEMIs produce characteristic ECG changes. Within hours of infarction, there are hyperacute T waves and ST segment elevation (except posterior infarcts, which produce ST depression and dominant R waves). Within 24 hours, the T wave inverts and the ST segment normalises. Within days to weeks, prominent Q waves develop and are usually the only long-term ECG change remaining following MI.
It should be noted that inferior MIs may damage the conduction system of the heart, producing heart blocks or bundle branch blocks. Therefore, infarction should also be suspected in any new left bundle branch blocks (LBBB).
In summary, ECG changes that are consistent with STEMI include:
- ST elevation (≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous praecordial leads)
- Posterior infarct (ST depression with dominant R wave in V1-V3)
- New LBBB
ECG changes occur in leads corresponding to the area of injury.
Blood tests (preform ASAP and repeat after 12 hours)
Cardiac enzymes leak out of infarcted myocytes and can be used as a marker of myocardial injury.
Troponins T and I are the most widely used marker given their good sensitivity and specificity profile. They rise 2-4 hours following MI and normalise after 10 days. False positives may be produced by pulmonary embolism, renal disease and pericarditis.
Creatine kinase is a non-specific marker that is found in the heart, brain and muscles. It rises 4-6 hours post-MI.
Further investigations
- Chest x-ray: may show pulmonary oedema
- Echocardiogram: Assess ventricular function and monitor complications
- Full blood count: leucocytosis, anaemia
- CRP/ESR: can be raised
- Cholesterol
- Glucose (check for diabetes)
Management
Acute management
Offer the below therapies for all types of ACS. In addition, patients with STEMI or high-risk features should be offered reperfusion therapy (see below).
- Glyceryl trinitrate (GTN)
- Analgesia and anti-emetic e.g. morphine and metoclopramide
- Aspirin
- Ticagrelor (or clopidogrel)
- Beta-blockers (if no hypotension present)
- Oxygen therapy (if hypoxaemic)
Reperfusion therapy in STEMI:
Primary percutaneous coronary intervention (PCI) should be offered to all patients with STEMI. If PCI cannot be provided within 120 minutes, provide thrombolysis until the patient can be transferred for PCI.
Reperfusion therapy should also be offered to patients with NSTEMI or unstable angina that have high-risk features.
Long-term management and secondary prevention
Lifestyle changes:
- Stop smoking
- Weight control
- Regular exercise
- Healthy diet
- Control any diabetes
- Control any hypertension
The following drugs should be offered for secondary cardiovascular prevention to all patients:
- Antiplatelets – both aspirin (indefinitely) and a second antiplatelet agent (for at least 12 months) e.g. clopidogrel, ticagrelor
- Beta-blockers; if contraindicated, provide a calcium channel blocker
- Angiotensin converting enzyme inhibitor (ACEi)
- Statin
Complications
Early
- Sudden cardiac death
- Arrhythmias
- Heart failure
- Pericarditis (usually 2-3 days post-MI)
- Mechanical complications occur due to fibrosis, including tear/rupture of:
- Ventricular septum → Ventricular septal defects and left-to-right shunting
- Papillary muscles → Mitral regurgitation → Pulmonary oedema
- Ventricular free wall → Tamponade (rapidly fatal)
Intermediate
- Deep vein thrombosis and pulmonary embolism
- Mural thrombosis (thrombus formation on infarcted ventricular walls) and systemic embolism
Late
- Ventricular aneurysm
- Dressler’s syndrome – pericarditis 2-10 weeks post-MI. Occurs in 5-10% of patients
- Cardioneurosis – anxiety surrounding heart conditions
Prognosis
Mortality ranges from 6-15% and is mostly due to arrhythmias (e.g. VF) or myocardial rupture.
Differential diagnosis
Very wide and includes all causes of chest pain.





0 Comments