

Introduction
Infective endocarditis is an infection of a heart valve, lining of a cardiac chamber or blood vessel. It is usually a bacterial infection and has a high rate of mortality.
Risk factors
- Congenital lesions e.g. Ventricular septal defects, bicuspid aortic valve, coarctation of aorta
- IV drug abuse
- Prosthetic valve replacement
- Cardiac/urinary catheterisation
- Invasive diagnostic or surgical procedures
- Colorectal cancer
Valves affected
Endocarditis usually produces valve regurgitation. Left-sided valves are most commonly affected, with the mitral valve being the commonest.
Right-sided lesions mostly occur following IV drug abuse. This is because blood from the peripheries, which can carry bacteria introduced by the needle, drains into the right side of the heart.
Causative organisms
Strep. viridians (50% of cases): dental procedures
Staph. aureus (20% of cases): IV drug abuse, prosthetic heart valves
Enterococcus faecalis (10% of cases): Urinary catheter, cystoscopy, colonoscopy
Staph. epidermidis: Prosthetic heart valves, dialysis
Strep. bovis: colorectal cancer
Fungi e.g. candida, aspergillus, histoplasma: Immunocompromised
HACEK organisms
Pathophysiology
Endocarditis usually arises as a consequence of 2 factors: abnormal cardiac endothelium (which facilitates organism adherence) and presence of pathogens in the bloodstream.
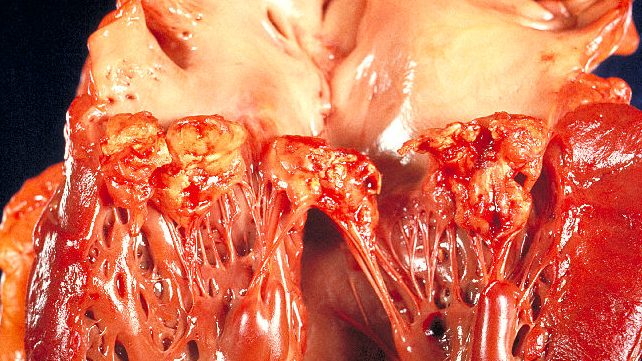
Circulating microorganisms can then adhere to cardiac tissues. Once adhered, they become encased in fibrin and platelets to grow rapidly into vegetations.
Clinical features
Presentation is variable and involves both structural and septic features. Common features include:
- Fever
- Malaise, anorexia and weight loss
- Embolic events
- New or changing murmurs
- Heart failure
Investigations
The most important investigations are blood cultures and echocardiograms.
- Blood cultures: take 3 samples of blood cultures. Must be taken before antibiotics are administered.
- Echocardiograms: definitive investigation for confirming vegetations.
Also consider:
- Urine dipstick – microscopic haematuria (glomerulonephritis due to circulating antigens)
- Fundoscopy – Roth’s spot
- ECG
- Routine blood tests – raised CRP/ESR, normocytic anaemia
- Chest x-ray
Diagnosing according to Duke’s criteria
A set of criteria for diagnosing infective endocarditis. Diagnose endocarditis if one of the following are met:
- 2 major criteria
- 1 major + 2 minor
- 5 minor
| Major | Minor |
| Typical organism on blood culture
Typical finding on echocardiogram e.g. vegetation, abscess, dehiscence | Atypical organism on blood culture
Atypical findings on echocardiogram Fever >38⁰C Embolic events e.g. arterial emboli, splinter haemorrhages Immunologic findings e.g. Osler’s nodes, Janeway lesions, Roth spots, Roth spots Predisposition e.g. prosthetic heart valve |
Management
Acutely, stabilise the patient and provide broad-spectrum antibiotics, such as IV gentamicin with benzylpenicillin; blood cultures should ideally be taken before starting antibiotics. Antibiotics should subsequently be tailored according to the sensitivity of organism and continued for 4-6 weeks.
Once the infection is eliminated, surgery should be offered to patients with large vegetations, new murmurs or abscesses.
Prognosis
20% fatality rate if treated. Mortality approaches 100% if untreated.





0 Comments