

Introduction
Numerous drugs act on or influence kidney function. This article provides a brief summary of clinically significant drugs (including diuretics and nephrotoxic drugs) that act on, impair or depend on renal function.
Diuretics
Diuretics are drugs that increase the production of urine. The following drugs have been arranged in order of their action on the nephron, from glomerulus to collecting ducts.
Osmotic diuretics
Example: Mannitol
Clinical uses include: Reduce intracranial and intraocular pressure
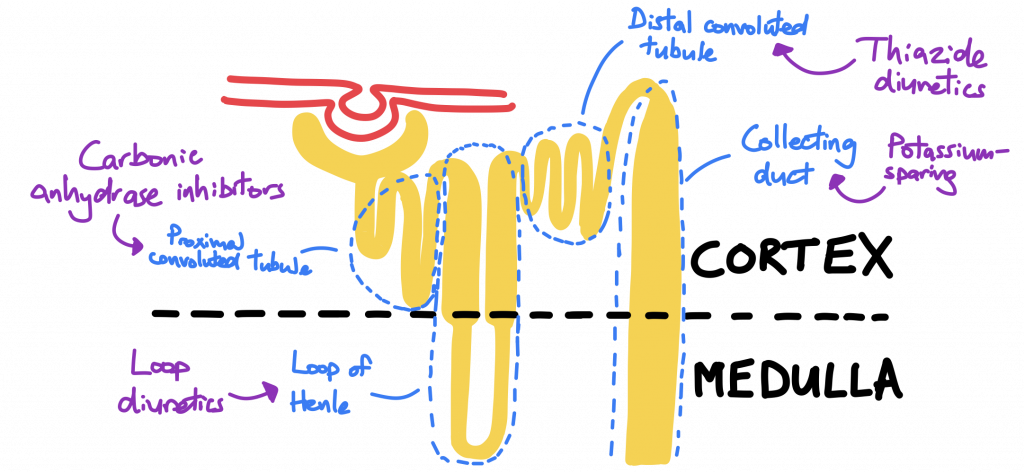
Carbonic anhydrase inhibitors
Example: Acetazolamide
Action: Act on proximal convoluted tubule to increase HCO3, Na+, K+ and water excretion.
Clinical uses include:
- Glaucoma
- High-altitude cerebral oedema (HACE)
Loop diuretics
Examples: furosemide, bumetanide
Action: Block Na+/K+/2Cl- cotransporter in the thick ascending loop of Henle. Increases excretion of sodium, potassium, magnesium and calcium.
Clinical uses include:
- Peripheral oedema
- Pulmonary oedema
- Hypertension in heart failure
- Severe hypercalcaemia
Thiazide diuretics
Example: bendroflumethiazide
Action: Block Na+/Cl- cotransporter in distal convoluted tubule. Increases excretion of sodium, potassium and magnesium, while calcium excretion is reduced.
Clinical uses include:
- Hypertension
- Prophylaxis against calcium kidney stones
- Nephrogenic diabetes insipidus
- Peripheral oedema
Potassium-sparing diuretics
Potassium-sparing diuretics can be either aldosterone inhibitors or epithelial sodium channel (ENaC) blockers:
- Aldosterone inhibitors: spironolactone
- Blockers of ENaC channels in the collecting ducts: amiloride, triamterene
Action: prevent sodium reabsorption in collecting tubule, consequently reducing water reabsorption and potassium excretion.
Clinical uses: used when diuresis is required when potassium needs to be retained; this is particularly useful when combined with loop or thiazide diuretics to counteract their hypokalaemic effects. Clinically used for treating:
- Heart failure
- Hypertension
- Liddle’s syndrome (ENaC blockers only)
Nephrotoxic drugs
Numerous drugs have an adverse effect on renal function. Several of these should be reviewed in the event of kidney disease and potentially withheld to avoid further deterioration in kidney function. Clinically significant examples include:
- Non-steroidal anti-inflammatory drugs (NSAIDs) (reduce renal filtration through afferent arteriolar constriction)
- ACE inhibitors/Angiotensin II receptor blockers (reduce renal filtration through efferent arteriolar dilation)
- Contrast dye e.g. dyes used in CT scans
- Antibiotics:
- Aminoglycosides
- Amphotericin B
- Lithium
- Methotrexate
- Ciclosporin
Drugs to consider withholding in kidney disease
Some drugs are renally excreted and should be reviewed in the event of kidney disease to avoid toxic accumulation. Examples include:
- Metformin (risk of lactic acidosis)
- Lithium
- Digoxin
Drugs to consider dose adjustment in kidney disease
In addition to the above, there are numerous drugs that may require dose adjustment in the presence of kidney disease. This includes:
- Antibiotics:
- Penicillins
- Tetracycline
- Aminoglycosides
- Trimethoprim
- Opioid analgesics (potential alternatives include oxycodone, fentanyl and alfentanil)
- Low-molecular-weight heparin
- Gabapentin
- Calcineurin inhibitors (e.g. tacrolimus)
- Methotrexate
- Allopurinol





0 Comments