

Introduction
The jugular venous pressure (JVP) refers to the pressure in the internal jugular veins. The JVP is an important sign of the central venous pressure (CVP), which is the pressure of the blood in the heart's right atrium. The height of the JVP waves reflects right heart pressure and function. An elevated JVP may indicate heart failure, constrictive pericarditis, or tricuspid stenosis. Low JVP may indicate hypovolemia, shock, or cardiac tamponade.
Practicalities of interpretation
Patients should be positioned at 45° to the horizontal when measuring the JVP. The JVP is easiest to observe along the sternocleidomastoid muscle.
Filling of the internal jugular 3 cm or higher above the angle Louis (sternal angle) is considered as elevated JVP.
Differences from carotid pulse
The JVP can be confused with the carotid pulse. Clinical features of the JVP include:
- Non-palpable
- Readily occludable – pressing on the vessel should stop the JVP. It can be observed that the vein fills from above
- Multiphasic – the JVP has 2 peaks for every heartbeat
- Decreases with respiration – inspiration decreases thoracic pressure, leading to increased venous return to the right heart and the pulmonary circulation
JVP waveforms
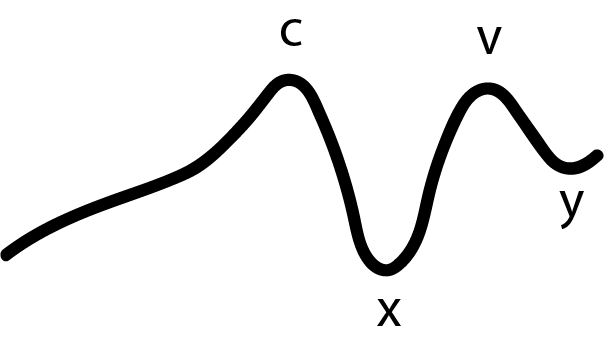
The waveforms of the JVP can be observed in invasive central venous pressure (CVP) monitoring. Changes in JVP waves may suggest pathology. Normal waveforms include:
a wave: first upward deflection in the waveform and is caused by the contraction of the right atrium during atrial systole.
c wave: second upward deflection in the waveform and is caused by the closure of the tricuspid valve during right ventricular contraction.
x descent: downward deflection caused by the downward pull on the right atrium during ventricular systole.
v wave: upward deflection caused by the filling of the right atrium against a closed tricuspid valve
y descent: downward deflection caused by the rapid emptying of the right atrium when tricuspid valve opens

Abnormal JVP waveforms
Absent a waves
Cause: Atrial fibrillation
Cannon a waves

Cannon a waves occur when the atria and ventricle contract simultaneously, producing a greatly elevated a wave.
Causes:
- Complete heart block
- Ventricular tachycardias
Large a wave

Causes:
- Tricuspid stenosis
- Pulmonary stenosis
- Pulmonary hypertension
Constrictive pericarditis vs Tamponade
The main method of differentiating tamponade from constrictive pericarditis on JVP is by observing the x and y descent. Tamponades produce sharp x descent only, whilst constrictive pericarditis produces sharp x and y descent.
Constrictive pericarditis
JVP features:
- Sharp x and y descent
- Large v wave
Tamponade
JVP features:
- Sharp x descent only
- Large v wave
Abnormal JVP height
Elevated JVP with normal waves
Causes:
- Fluid overload
- Heart failure
Elevated JVP with no waves present
Cause: Superior vena cava obstruction
Absent JVP
Cause: Hypovolaemia
Kussmaul's sign
Normally, the JVP should go down with inspiration as a result of the drop in intrathoracic pressure. Kussmaul's sign is an abnormal finding that refers to the JVP paradoxically rising with inspiration. It is seen in conditions affecting right heart function. During inspiration in right heart dysfunction, there is an increase in venous return but the heart cannot effectively pump it through the pulmonary circulation, leading to JVP elevation.
Causes:
- Tamponade
- Constrictive pericarditis
- Right heart failure





0 Comments